2 December 2021
Lies, Damned Lies and Coronavirus
The new variant
by David Chilvers
There has been a lot of excitement in the past few days over the discovery of a new variant of COVID-19 in southern Africa. First identified on Tuesday, by Thursday it had become a Variant of Concern (VOC) and given the name Omicron – the fifteenth letter of the Greek alphabet, assigned to the thirteenth VOC. Two letters were missed out; Nu, as it was felt this was too close to “new” and Xi, as this is the name of the Chinese President. It clearly didn’t dawn on the World Health Organisation, which assigns the names, that Omicron is an anagram of moronic.
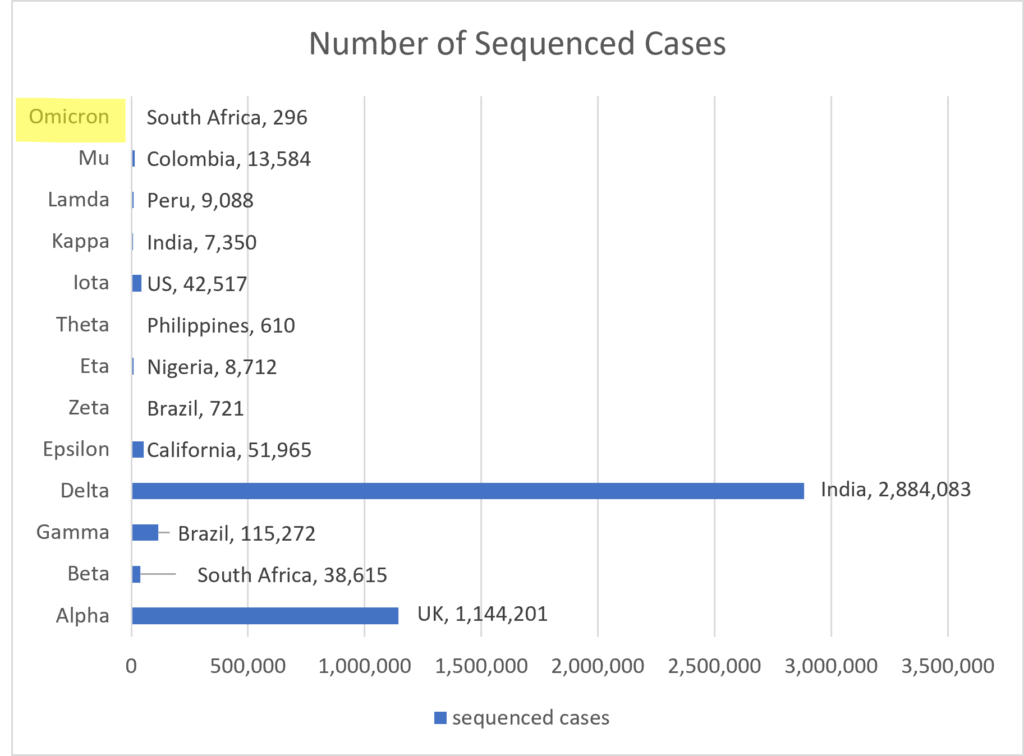
Regular readers will recall that back in June the Shaw Sheet exclusively announced the discovery of the Omega variant among nomadic tribesmen in the Gobi desert. This was, of course, a spoof, but it is worth recalling that of the previous twelve VOCs, only two – Alpha and Delta – developed in significant numbers around the world. These two variants account for 93% of all positive COVID tests that have been genome sequenced.
The speed at which the assignment of VOC status to Omicron has happened reflects concern that this variant may be more of a threat than most of the preceding twelve. We will have to wait and see what happens with Omicron but the lack of evidence so far did not prevent the doom-mongers from coming out in force.
On Friday, Sajid Javid, the UK Health Secretary made a statement that “while hard data is presently lacking, early indications show this variant may be more transmissible than the Delta variant, and current vaccines may be less effective against it. It may also impact the effectiveness of one of our major treatments, Ronapreve.” I have emboldened key words to confirm that in the absence of any hard facts, our Health Secretary can still suggest that this is of great concern. He could have used “may not” instead of “may” and the statement would have been equally valid but much less threatening (and of course much less newsworthy).
In contrast to the negative assessment made by the UK Health Secretary, others were more balanced in their views. Professor Chris Whitty said it was impossible to know what measures might be needed to deal with Omicron. “There’s an awful lot we don’t know and I think it’s probably not helpful to speculate on how big a threat the variant will be”. Sir John Bell, Regius professor of medicine at Oxford University, told Times Radio: “Calm down, put your seatbelt on, it’ll be fine.”
At a press conference on Saturday, Boris Johnson announced that face masks would again be mandatory on public transport and in retail outlets, but not in hospitality venues. So, I can watch West Ham play football with 50k others and not wear a mask. I can spend hours in a crowded pub before the match and not wear a mask. I can go into a crowded restaurant after the match and not wear a mask. I can even go into the Westfield nightclub later on and dance in close proximity to lots of people and not wear a mask. But if I go into a shop in the Westfield shopping mall, I must wear a mask. The proximity of other people will be less in the shops than in the football stadium, the pub, the restaurant and the nightclub but I must wear a mask in the former not the latter. Let’s be honest, this is not science. It’s a token gesture to say the Government is doing something without seriously harming the economy; it’s a decision based upon economics not science or medicine.
In spite of the Health Secretary’s statement, there is some hard data in the public domain; the progress of each variant in each country is updated daily on the Gisead website and data on the number of positive tests (“cases”), hospitalisations, deaths and vaccinations in most countries is updated daily on the Our World in data website. This gives some useful information in the countries where the Omicron variant is present and provides some basis for answering the question of how much of a threat is it likely to be?
Up until 23 November, there had been 81 positive COVID tests that had been genome sequenced and assigned to Omicron – 60 in South Africa, 19 in Botswana and 2 elsewhere. By 30 November, there had been 172 Omicron cases in South Africa – up 112 – and 19 still in Botswana (this might reflect the slowness of reporting there) and 33 had emerged in Ghana in just a few days. The total had increased from 81 to 296 in a week.
In Botswana, 8% of the population have had COVID-19 and the vaccination rate is around 1 dose per 100 people. There is thus low acquired immunity, either through disease or vaccination and these are exactly the conditions the WHO outlined where a new variant might develop. 19% of genome sequenced cases in Botswana in the past four weeks have been the Omicron variant. The first evidence of an Omicron case in Botswana is now believed to have been on 11 November and so if this variant is much more transmissible than previous variants, we might expect to see the number of positive tests – “cases” – taking off. This is what has actually happened according to the Our World in data database:
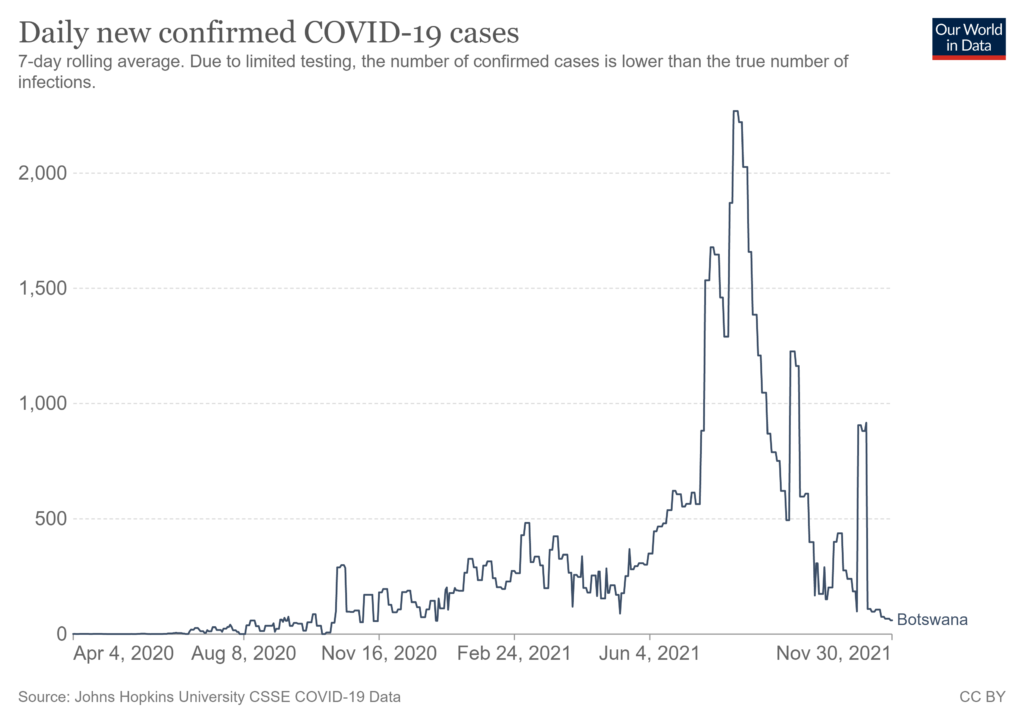
There was a surge between November 3 and November 10 but this was before Omicron was detected. Since then, cases have steadily fallen. So, in a country with low immunity, the appearance of a new variant of concern has not led to any increases in case numbers, in fact quite the opposite.
In Ghana, all the positive tests genome sequenced in the past few days have been the Omicron variant. 100% sounds scary – clearly the dominant strain very quickly – but what has happened to cases overall.
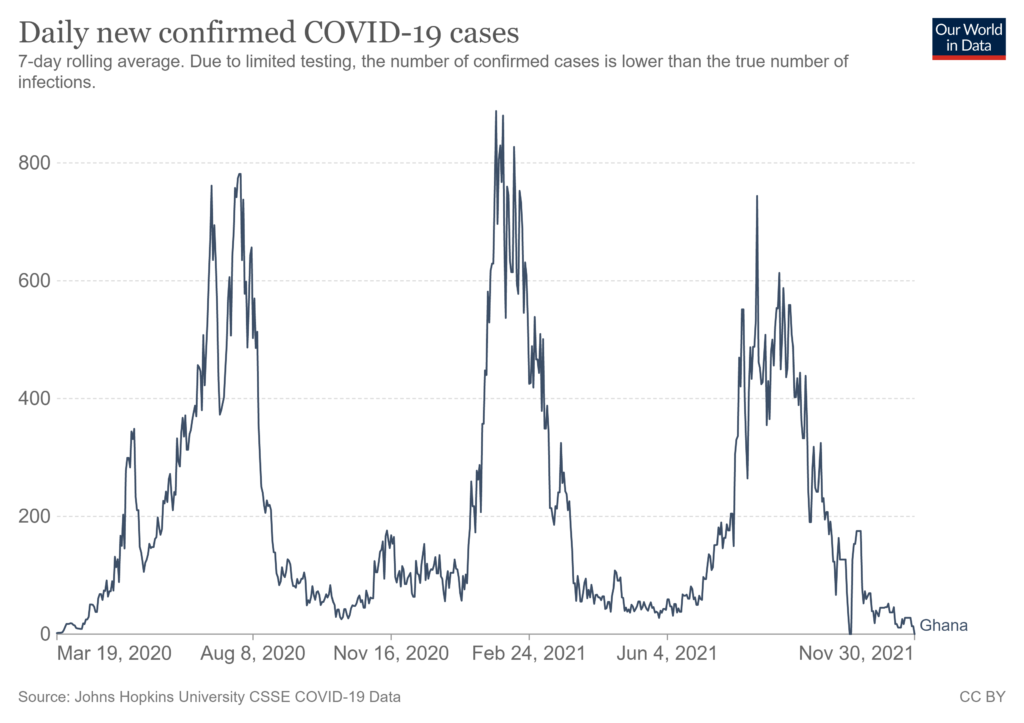
A very similar pattern to Botswana – hardly any cases but all of those genome sequenced are the Omicron variant. 100% is obviously large but if it is applied to a small number, that’s still a small number.
In South Africa, 5% of the population have had COVID-19 and there have been 31 vaccinations per 100 people. This means a minority of the population has acquired immunity either through infection or vaccination. As Ed Conway of Sky News (alone of the media ready to look for data) commented on Tuesday, around 80% of the cases genome sequenced in the past four weeks have been the Omicron variant, so it has quickly become the dominant variant.
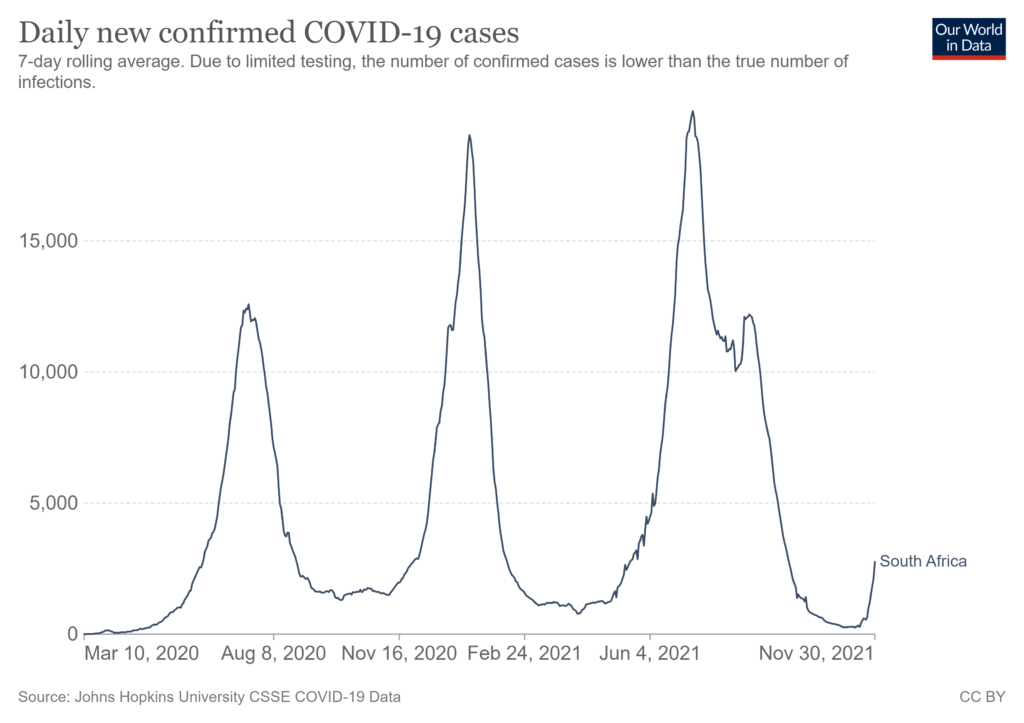
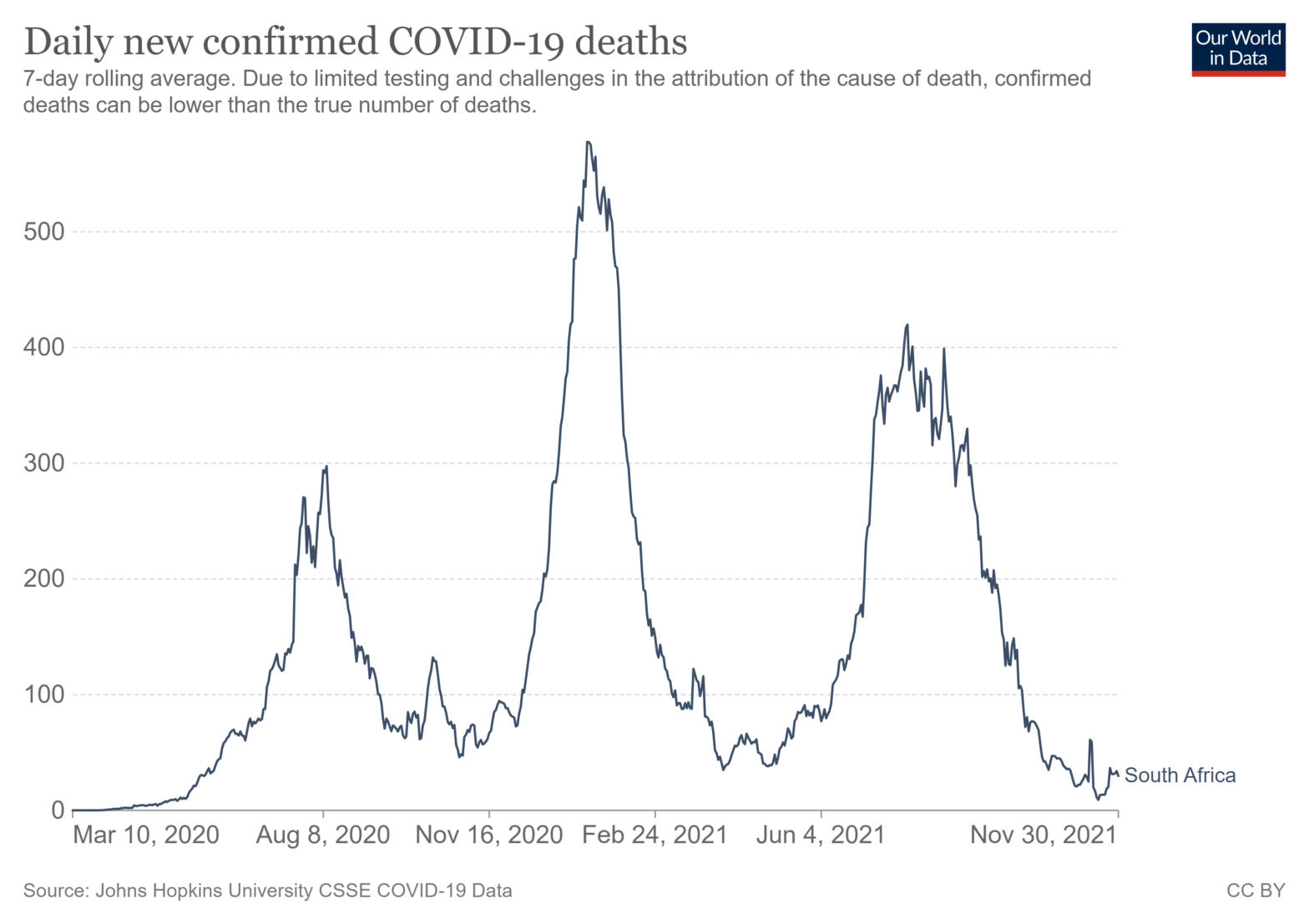
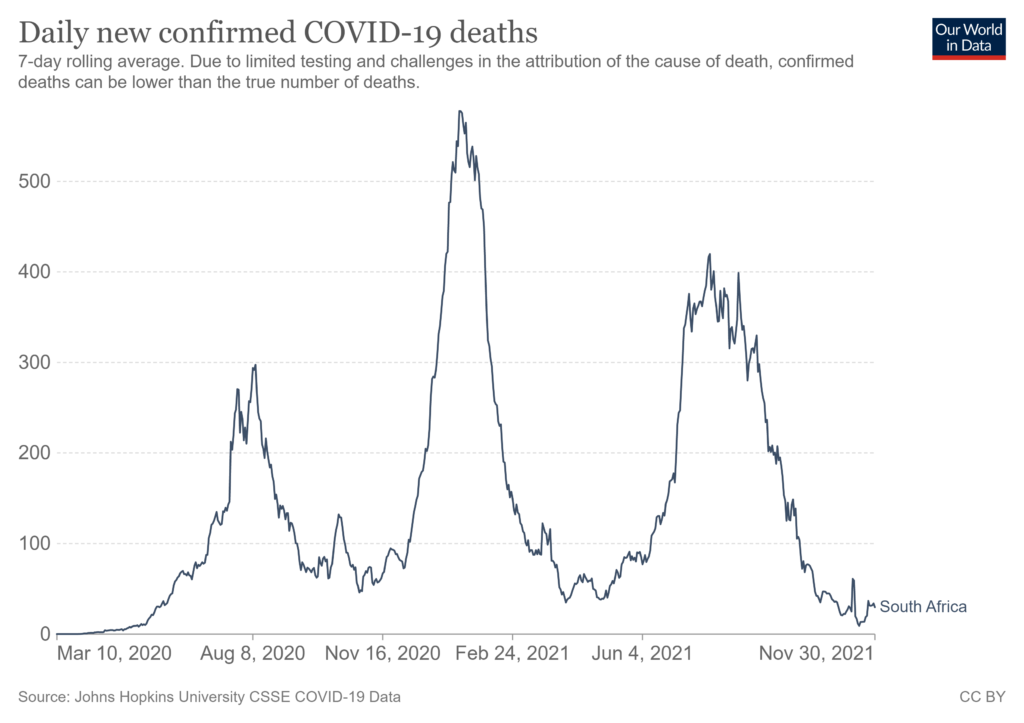
In contrast to Botswana and Ghana, there has been a rise in the number of positive tests in recent days but to a level of under 20% of the peak in June this year. This could be the start of another wave and the upward trajectory is certainly quite steep. However, Dr Angelique Coetzee, the South African doctor who first spotted the new Covid variant Omicron, says the patients seen so far have had “extremely mild symptoms” but more time is needed before we know the seriousness of the disease for vulnerable people. Certainly, there is no rise in deaths yet but it perhaps early to tell this given the variant has been around for only around 3 weeks.
It is early days yet but time will tell how this develops. What I do find concerning is that all this data is available on public websites, but none of it appears in the UK mainstream media. We have generalities about cases taking off in Africa but no hard data in which to put this in context, which is available if you bother to look for it.
Finally, it is worth looking back at what happened with the Beta variant, which also originated in South Africa. When it was first identified in the UK in April this year, the government recommended surge testing in areas where it had been found, to help stop the spread. Surge testing can help identify both asymptomatic and symptomatic cases and reduce transmission of the new variant. The Beta variant had more mutations than previous variants and was thought to be far more transmissible, but not more lethal, than other variants of the coronavirus. There’s was also emerging evidence to suggest it was less susceptible to immunity induced by the Covid-19 vaccines; so, more mutations, more transmissible and more likely to evade the existing vaccines. This all sounds very similar to the situation now with the Omicron variant and the actions being taken. In the end, the current total number of cases of the Beta variant identified in the UK to date is 1,077 and there have been hardly any cases since June. In short, the programme the Government put in place in April to contain the Beta variant resulted in a successful suppression of that strain; let’s hope the similar programme being put into place now will have the same effect.
This article is one of a series, the previous article on a possible wave 4 is here.