13 May 2021
Lies, Damned Lies and Coronavirus
False positives
by David Chilvers
 On Monday, Boris Johnson confirmed that Stage 3 of the COVID roadmap would be implemented as planned. This involves indoor socialising, up to a maximum of six people, and represents a further step towards normality for large parts of the hospitality industry. Travel to 12 green list countries will also be permitted, but most of this list has yet to allow UK citizens to visit, which leaves a few islands in the South Atlantic as the current modest beneficiaries of this relaxation.
On Monday, Boris Johnson confirmed that Stage 3 of the COVID roadmap would be implemented as planned. This involves indoor socialising, up to a maximum of six people, and represents a further step towards normality for large parts of the hospitality industry. Travel to 12 green list countries will also be permitted, but most of this list has yet to allow UK citizens to visit, which leaves a few islands in the South Atlantic as the current modest beneficiaries of this relaxation.
“Data not dates” has been the mantra driving the changes and it is certainly the case that most of the important metrics continue to decline from the position a month ago (all data is for the UK and is a seven-day moving average on 1st May compared to 1st April):
- The number of positive tests was 2,010 on 1st May compared to 3,153 on 1st April, a fall of 36%
- The number of hospital admissions was 108 on 1st May compared to 238 on 1st April, a fall of 54%
- The number of patients in hospital with coronavirus was 1,357 on 1st May compared to 3,618 on 1st April, a fall of 63%
- The number of deaths within 28 days of a positive test was 9 on 1st May compared to 33 on 1st April, a fall of 71%
So, over the course of the past month, deaths and numbers in hospital have been cut by about two thirds, hospital admissions by about half and the number of positive tests by about one third. This is the impact that the medics and scientists predicted from the vaccine rollout, with the biggest impact on the most severe cases but some increasing evidence that there is a vaccine impact on infection as well as severity of symptoms.
It is clear, however, that the slowdown in the number of positive tests has started to plateau over recent weeks. The chart below shows that the numbers have been around 2,000 for a couple of weeks now against a fairly constant level of testing (the number of positive test results will go up and down as the number of tests varies):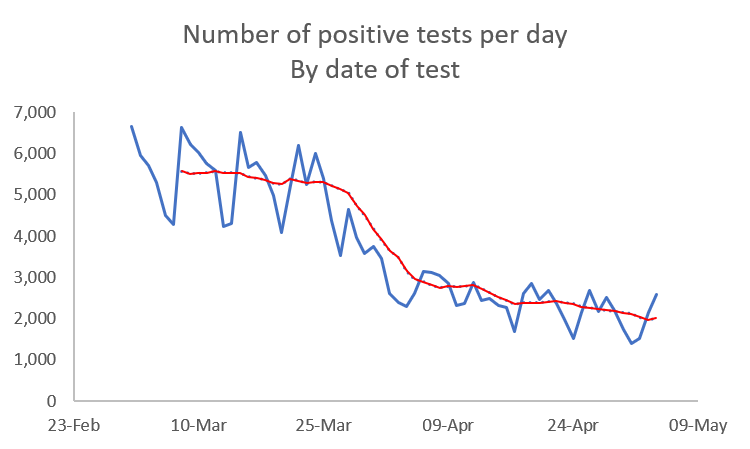
One view is that the relaxations of 29 March and 12 April will increase social interaction and that this will increase infection but that the rollout of the vaccine programme will counteract this. But there is another hypothesis, which is that many of the positive tests are now false positives and as a result it is unlikely that the number of positive tests will fall much further (unless the level of testing drops – as Donald Trump once remarked, the easy way to eliminate coronavirus was to stop testing as there would then be no positive test results and thus no “cases”).
False positives occur when a test gives a positive result but the individual does not have the disease. Such outcomes will inevitably occur with most testing regimes, particularly when done by an untrained person. Most LFD[1] tests and some PCR[2] tests involve the individual administering the test themselves. Having undertaken an LFD test myself recently, I can report that the instructions are complex and might lead to error. There is also the possibility of analysis errors, at home with the LFD test and in the Lighthouse labs that process many of the PCR tests; the sheer volume of tests will lead to a small number of mistakes.
In a recent document, the Office for National Statistics provides data on the likely level of false positives as follows:
- LFD tests: from 0.03% to 0.10%
- PCR tests: from 0.5% to 1.9%
These are low numbers, but the current low prevalence of COVID-19 means that the positivity rates (the % of tests that show a positive result) are close to these numbers: 0.07% for LFD tests and 0.59% for PCR tests. If we took the lowest false positive estimates from the ONS report (0.03% and 0.5%), false positives would represent 45% of positive LFD results during the last month and 85% of positive PCR results.
Looked at another way, of the average 971,212 tests per day undertaken during April, we would expect 1,272 false positives compared to the 1,727 total positive cases recorded, some 72% of the total; most positive cases being recorded at the current low levels of infection are likely to be false positives.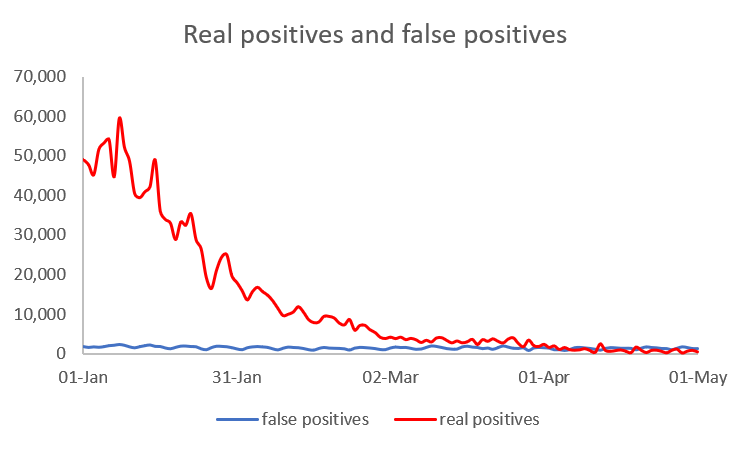 The above graph shows the number of false positives and real positives since the start of 2021. At the start of the year, the number of false positives cannot really be seen. However, if we look at data for the last month, a very different picture emerges.
The above graph shows the number of false positives and real positives since the start of 2021. At the start of the year, the number of false positives cannot really be seen. However, if we look at data for the last month, a very different picture emerges.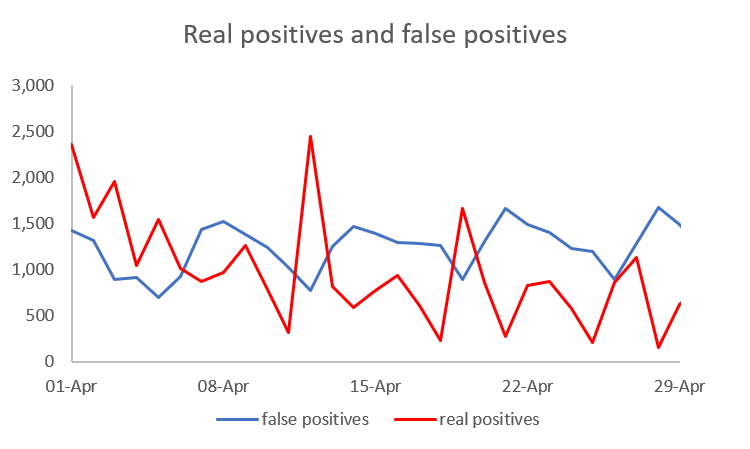 For the past few weeks, the number of false positives has exceeded the number of real positives on most days (assuming a constant % of false positives for LFD and PCR tests as detailed above).
For the past few weeks, the number of false positives has exceeded the number of real positives on most days (assuming a constant % of false positives for LFD and PCR tests as detailed above).
The same phenomenon occurred in July/August last year, when again the level of infection was low. Testing was also much lower at under 200k tests per day, all PCR, but the pattern of false positives exceeding real positives on most days is apparent (estimated real positives fall below 0 on a few days, as the method of estimation assumes the % of false positives is constant throughout, when in reality it will vary from day to day).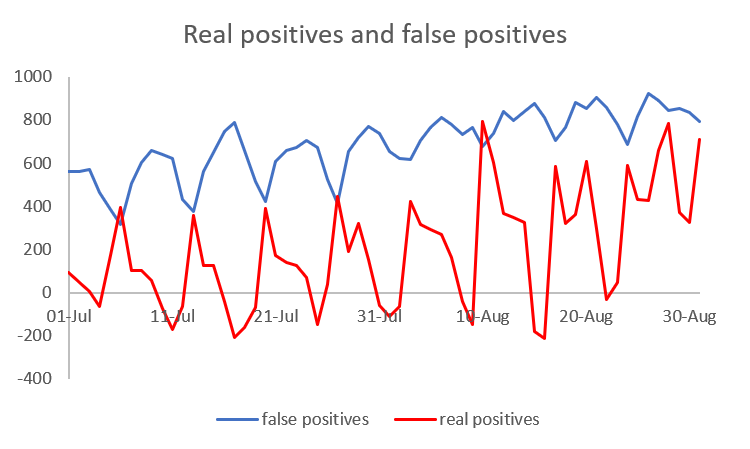 This raises the question of whether the current high level of national testing is an appropriate strategy. Testing those attending specific events or in an area where a new variant has been detected all makes sense but continuing the expense of around one million tests a day when most of the positive results are false positives hardly seems value for the estimated £15 million per day or £100 million per week cost of these tests. Curtailing this expenditure would enable the Overseas Aid budget to be returned to 0.7% of GDP or could start making inroads into the large national debt incurred during the pandemic.
This raises the question of whether the current high level of national testing is an appropriate strategy. Testing those attending specific events or in an area where a new variant has been detected all makes sense but continuing the expense of around one million tests a day when most of the positive results are false positives hardly seems value for the estimated £15 million per day or £100 million per week cost of these tests. Curtailing this expenditure would enable the Overseas Aid budget to be returned to 0.7% of GDP or could start making inroads into the large national debt incurred during the pandemic.
This article is one of a series, find last week’s on a possible third wave is here.
[1] Lateral Flow Device – Lateral flow tests are administered at home or in schools and other places on a sample from the mouth. A special strip of paper coated with antibodies responds to parts of the Coronavirus by showing a marker; a check marker to confirms that it is working properly.
[2] Polymerase Chain Reaction – the test for those with symptoms – a more expensive, more complex & more accurate test than LFD which multiplies the amount of Covid-19 RNA in the sample so that it is more easily detected.